
I am newly diagnosed with CML. I'll be 69 next month and until this surprise, I thought I was in excellent health. I have been taking 80 mg daily of Atorvastatin (Liptor) because of cholesterol issues. Liptor has interactions with Imatinib. PCP is substituting Crestor at a lower dose for now. Crestor is perhaps the most dangerous of statins. Anybody faced a similar issue? Would appreciate some wisdom here.
You are here
Imatinib and Statins
Categories:


Hi Rick,
I have a lot of experience over 12 years with the use of statins and the possible interaction with imatinib
If you google "Drug interactions with tkis" you may well be able to source an article by Haouala and others titled "Drug interactions with the tyrosine kinase inhibitors-imatinib,dasatinib and nilotinib"
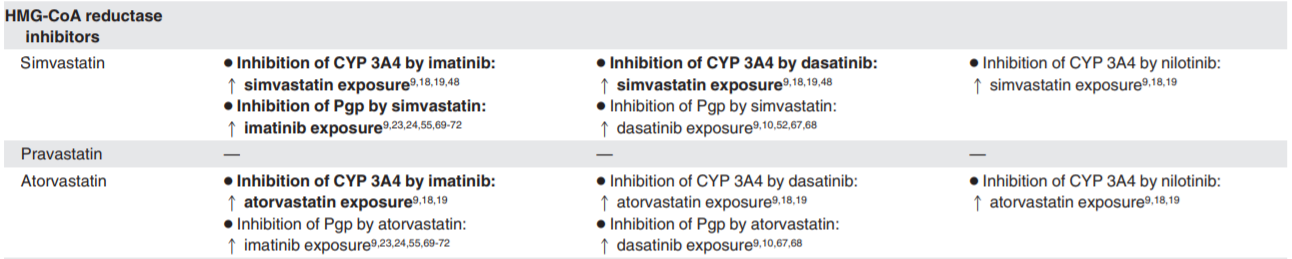
Simvastatin should not be combined with imatinib as it leads to higher exposure of itself and as well it leads to higher imatinib exposure-side effects might be muscular inflammation or myositis.Likewise Atorvastatin (Lipitor) has similar effects.
Imatinib will tolerate Pravastatin so I advise you to insist that you be prescribed this .The article that I noted above does not have an entry indicating any interaction between Rosuvastatin (Crestor) and imatinib but there may at the moment be insufficient evidence available
If you ever have to take medication such as Losartin in order to control blood pressure do not do so-take Candesartan instead
I am now with a different haematologist and a few days ago we reviewed the medicines that I am taking alongside my imatinib and he approved of Pravastatin etc;he advised never to accept live vaccines say for yellow fever .Last year I was offered the shingles jab but declined it as it could lead to a serious infection if given alongside imatinib.
Most non specialist doctors do not know about nor do they check interactions with tkis.
There have been previous threads here on this forum on drug interaction
I trust this helps
Regards
John
Hi Rick,
I have a lot of experience over 12 years with the use of statins and the possible interaction with imatinib
If you google "Drug interactions with tkis" you may well be able to source an article by Haouala and others titled "Drug interactions with the tyrosine kinase inhibitors-imatinib,dasatinib and nilotinib"
Simvastatin should not be combined with imatinib as it leads to higher exposure of itself and as well it leads to higher imatinib exposure-side effects might be muscular inflammation or myositis.Likewise Atorvastatin (Lipitor) has similar effects.
Imatinib will tolerate Pravastatin so I advise you to insist that you be prescribed this .The article that I noted above does not have an entry indicating any interaction between Rosuvastatin (Crestor) and imatinib but there may at the moment be insufficient evidence available
If you ever have to take medication such as Losartin in order to control blood pressure do not do so-take Candesartan instead
I am now with a different haematologist and a few days ago we reviewed the medicines that I am taking alongside my imatinib and he approved of Pravastatin etc;he advised never to accept live vaccines say for yellow fever .Last year I was offered the shingles jab but declined it as it could lead to a serious infection if given alongside imatinib.
Most non specialist doctors do not know about nor do they check interactions with tkis.
There have been previous threads here on this forum on drug interaction
I trust this helps
Regards
John

Hi Statin Takers
I used to take simvastatin just because my GP thought everyone aged over 40 yrs should as a precaution. . After taking imatinib for about 3 years I experienced burning, pins and needles and then feeling as if I was walking on broken glass - the soles of my feet were very painful. At a CML conference in Cardiff in 2011(?) I asked Prof O Neill ( a CML specialist from Newcastle Cancer Research Institute I believe ) about taking statins and imatinib. He advised that people on TKIs should very cautious about statins as they can increase side effects. I stopped taking simvastatin and my feet were just fine after 3 days. No more statins for me.
Just a personal experience,
best
Chrissie
I saw my GP this morning. I am told that Simvastatin should not be taken alongside Imatinib and certainly not greater than 10 mg. My haematologist does not like statins but recognises that there may be a place for them for people like me with diabetes. The GP decision is that I should move to Pravastatin 40 mg which is permitted alongside Imatinib.

The dreaded CYP3A4 interaction at work ... it's the same underlying reason that we must avoid grapefruit.
Here is a very useful article in Blood journal - a source you can trust - that has a lengthy table which details drug interactions with imatinib, nilotinib and dasatinib:
http://www.bloodjournal.org/content/bloodjournal/117/8/e75.full.pdf
As you can see from this table, pravastatin does certainly look like the best bet.
David.

Hi All,
As someone who is just trying to get my head around all of this could someone explain a little bit about this table? It’s obvious that certain drugs react with the TKIs but what are the different issues with a decreased uptake of the drug and also an increased uptake? The decrease seems fairly obvious, but does an increased uptake put strain on your body and maybe add to the side affects? Simple terms at the moment is best for me.
I'm particularly interested as I’m UK based, on imatinib 400g / day and have been taking this for just under two months now. I had no side affects until just recently where terrible leg pain (bone and muscle) has started. It looks like ibuprofen is out but paracetamol and aspirin are ok? I was actually feeling better than I had for a long long time, mainly due to an increase in hb from 8.6 to 12.5 but this leg pain has been a real set back.
Many thanks
Hi David, the simplest way I can explain how other drugs increase uptake is the same mechanism behind why we must avoid grapefruit.
There’s an enzyme in your body called CYP3A4. This enzyme is important in how imatinib, and other TKIs, gets broken down. To break down grapefruit juice (and some other drugs) this same enzyme is needed. Since there isn’t an unlimited supply of this enzyme in your body, if you drink grapefruit juice all the available enzyme is used up, so when you take your medication it remains active for longer than it should as there’s no enzyme left to break it down until your body can make more. Increased exposure over time can cause problems like making side effects worse, or introducing new side effects.
I hope that makes sense?
In terms of painkillers, regular use of paracetamol can be hard on your liver. Ibuprofen is tough on your stomach too. When I had a lot of pain because of CML my doctor prescribed codeine as it is easily metabolised and not tough on your body
David.
That’s a real help, thank you very much David. Certainly explained in a way I can understand before I’ve managed to do more in depth reading on the subject.
I think I’m going to see if my GP will prescribe some codeine for the short term until I can discuss things further with my consultant. I believe this pain I’m experiencing is fairly common on Imatinib and subsides over time in many people.
Regards
